INTRODUCTION
Humans show near-24-h rhythms in both physiological traits, such as cortisol, melatonin, and core body temperature, as well as behavioral traits, including the daily cycle of sleep and wakefulness [1,2]. In modern society, disruptions in circadian rhythms and sleep patterns are becoming serious concerns. Sleep disorders, such as insomnia and narcolepsy, cause many adverse health effects worldwide and are widespread among the general population in modern society [3,4]. Previous studies have reported that 50-70 million adults suffer from sleep disorders, with insomnia being the most common disorder in the United States [3,5]. According to a nationwide study in Japan, prevalence of insomnia was 12.2% among men and 14.6% among women [6]. Furthermore, a study conducted in South Korea, based on national data, reported an increased prevalence of insomnia over the last decade, increasing from 3.1% to 7.2% among females and from 1.62% to 4.32% among males [7]. Many studies have shown that a sedentary lifestyle disrupts the circadian rhythm and negatively affects sleep quality [8].
A sedentary lifestyle is a major concern in modern society [9], as it reduces sleep quality and poses a substantial threat to global public health [10,11]. Many studies have comprehensively evaluated sleep quality by measuring several factors, including non-rapid eye movement (NREM) sleep, sleep stages, sleep onset latency, and sleep efficiency, via polysomnography (PSG). Sleep quality can also be evaluated using actigraphy accelerometers and the Pittsburgh Sleep Quality Index (PSQI) questionnaire. In addition to reducing sleep quality, physical inactivity tends to increase the risk of obesity and type 2 diabetes, often resulting in premature death [10]. Previous studies have demonstrated a positive association between increased physical activity and reduced sedentary behavior and sleep quality [3,11]. Mendham et al. reported that 12 weeks of moderate- to vigorous-intensity combined resistance and aerobic training (40-60 min, 4 days/week) improved sleep efficiency (p = 0.005), as measured using the PSQI, in female adults [12]. Furthermore, 6 months of 50% VO2 peak ergometer and treadmill exercise (12 kcal per body weight/week, 3-4 days/week) significantly improved subjective sleep quality in postmenopausal women, with even a low dose of exercise substantially reducing the likelihood of significant sleep disturbance [13]. However, some studies have reported that while morning exercise can improve sleep quality, evening exercise has the opposite effect [14-17]. Tworoger et al. reported that postmenopausal women who exercised for >225 min in the evening had an increased risk of experiencing difficulty falling asleep [17]. Therefore, it is necessary to consider factors such as the timing, duration, frequency, intensity, and type of exercise when reviewing its effects on sleep quality.
Humans possess physiological circadian rhythms that are closely associated with sleep quality [2]. The hormones cortisol and melatonin and core body temperature show notable circadian rhythms [18,19]. Core body temperature decreases at night and increases during daytime. Cortisol and melatonin are counter-regulatory hormones; melatonin levels increase at night, when cortisol levels decrease to their lowest point, and cortisol levels increase to their highest point in the morning, when melatonin levels decrease to their lowest. Abnormal melatonin and cortisol rhythms can cause sleep problems [20,21]. Cortisol, a prominent hormone in circadian rhythms, reacts rapidly to exercise [22], stimulating the sympathetic nervous system as its concentration rapidly increases [23]. Kanaley et al. reported that evening exercise significantly increased cortisol concentrations compared to morning exercise [24]. Additionally, cortisol concentration significantly increases after moderate-intensity exercise compared with low-intensity exercise [25]. To the best of our knowledge, no previous review has summarized circadian rhythms and sleep quality with respect to the intensity and timing of various exercise regimens.
We systematically reviewed studies that measured the effects of exercise intensity and timing on physiological circadian rhythms and sleep quality.
METHODS
Search strategy and eligibility criteria
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for searching, selecting, collecting, and analyzing data [26]. We identified studies published between January 2000 and April 2023 using the PubMed, Web of Science, Embase, and Science Direct electronic databases. Our review focused solely on published articles, and we did not contact authors regarding unpublished articles or results. The participant, intervention, comparison, and outcome (PICO) characteristics were: (1) adults aged <65 years; (2) exercise treatment of any duration; (3) controls receiving no exercise treatment or different types of exercise (pre-exercise baseline); (4) cortisol, melatonin, or body temperature measurement, and subjective or objective sleep quality assessments. The search items included a combination of medical subject headings (MeSH terms) and the following freetext words: (1) circadian rhythm, cortisol, melatonin, or core body temperature; (2) sleep quality; and (3) exercise, physical activity, or training.
The inclusion criteria were as follows: (1) original research articles; (2) studies that physiologically measured cortisol, melatonin, or core body temperature; (3) adults of either sex aged < 65 years without metabolic syndrome or cancer; and (4) studies published in English. The exclusion criteria were as follows: (1) studies that included participants with metabolic syndrome or cancer; (2) studies that did not assess physiological measurements of circadian rhythm hormones or core body temperature; (3) studies that reported only the quality of sleep without circadian hormone measurements; (4) observational and longitudinal studies; (5) studies that did not describe the exact intensity and time of exercise; and (6) studies conducted before January 2000.
Study selection
Duplicate studies were removed using EndNote (version 20; Clarivate Analytics, Philadelphia, PA, USA) [27]. Two independent reviewers performed the search and selected studies. Disagreements between reviewers were resolved through discussion. Additionally, the titles and abstracts of the studies were searched and screened, and both the independent reviewers evaluated the full texts of the articles for inclusion during the second screening step. Discussions with a third reviewer were held when the two reviewers failed to reach an agreement. Studies were excluded if the outcomes of interest were not measured and the results for the outcome of interest were not reported.
Data extraction and conversions
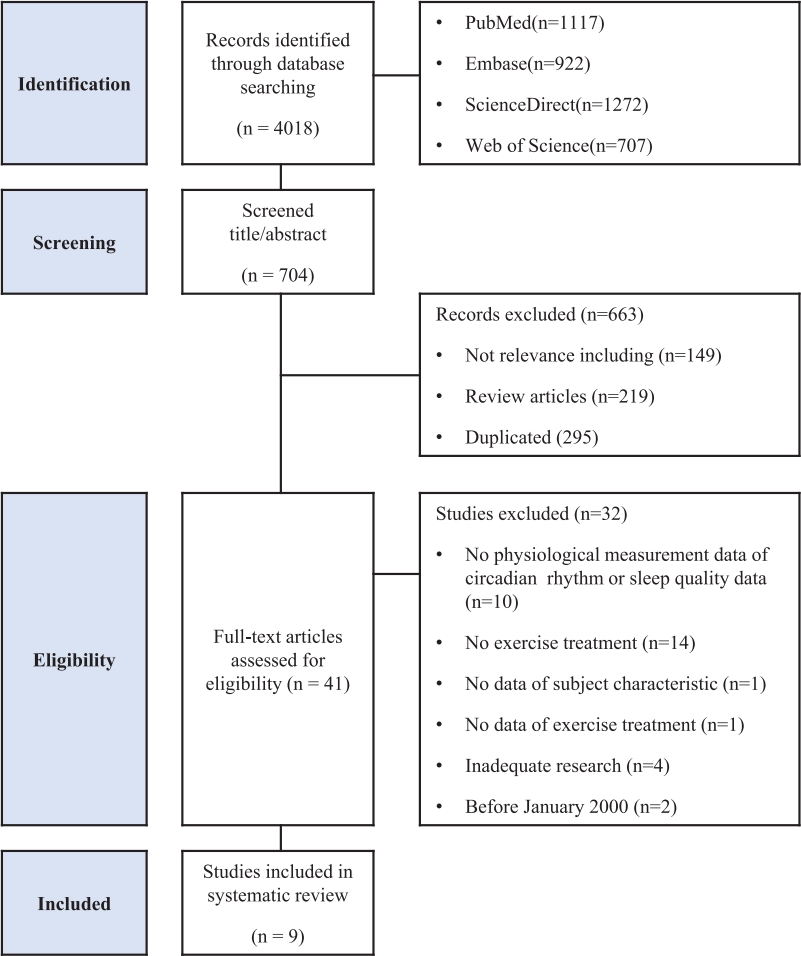
The screening and identification of studies included in this review are shown in Figure 1. Two authors independently extracted the data using Excel. Another reviewer double-checked the extracted data and resolved discrepancies through consensus-meeting discussions. The extracted study data included the year of publication, number of participants, participant characteristics (age, sex, health status), exercise treatment information (type, length, duration, frequency, intensity, and timing), physiological measurements of circadian measurements (blood cortisol, salivary cortisol, urine cortisol, plasma melatonin, core body temperature, area under curve of hormone concentration, and cortisol awakening response [CAR]), and subjective or objective measures of sleep quality (PSG, PSQI, and actigraphy). The decimal places for age data were rounded off.
Study identification and selection
A total of 4018 studies were retrieved after searching the four databases. After reviewing the titles and abstracts of the studies, 3316 studies were excluded from the analysis. An additional 663 articles were excluded after eliminating duplicates and reviews. A total of 12 studies were included in the final analysis, after excluding 32 studies that did not measure or report the results of interest, had no exercise treatment, had no physiological circadian rhythm measurement, or were published before January 2000.
Quality assessment
We used the Risk of Bias 2 (RoB2) tool, recommended by the Cochrane Systematic Review Manual (5.4.0) [28,29], to assess the risk of bias in the included randomized controlled trials (RCTs). We used the Risk of Bias in Non-Randomized Studies-of Interventions (ROBINS-I tool) to assess the risk of bias in the included non-RCTs [30,31]. This tool was used to evaluate the quality of the literature. Two reviewers (NHK and SJK) conducted independent assessments of the risk of bias for each included study, categorizing them as ŌĆ£low risk,ŌĆØ ŌĆ£some concerns,ŌĆØ or ŌĆ£high risk.ŌĆØ Another reviewer (JHP) reviewed the results and resolved disagreements.
RESULTS
Study characteristics
We investigated the effects of exercise timing and intensity on circadian rhythms and sleep quality in adult participants aged 18-65 years (n=201 participants; 77.1% male). All the participants included in this systematic review were male and female adults without cardiovascular disease, cancer, diabetes, or physical illnesses. Sex distribution showed a higher male representation (n=155 participants), with two studies examining both sexes [32,33], six including only male participants [34-39], and one study including only female participants [40]. One study included post-menopausal females [40]. Two of the 11 study subjects experienced sleep disturbances [37,40], and the subjects of one study had chronic primary insomnia [33]. The participants in one of the 11 studies were non-professional athletes [38]. One of the study participants was a patient with depression [32].
All the studies evaluated sleep quality based on circadian rhythms. Seven studies measured sleep quality using PSG [32-34,36,37,39], one study assessed sleep quality using actigraphy [38], and four studies assessed sleep quality using PSQI [32,33,35,40]. Four studies measured melatonin levels [34,36,37,40], five measured cortisol levels [32,33,35,37,38], and one evaluated core body temperature [39]. One study assessed both melatonin and cortisol levels [37], and another measured melatonin rhythm and core body temperature [36]. Table 1 presents a detailed list of studies, including authors, participants, exercise intensity, exercise length, exercise timing, exercise frequency, and duration, comparison, and outcomes of circadian rhythm and sleep quality.
Summary of outcomes
Effect of exercise timing on circadian rhythm and sleep quality
One study compared the effects of exercise timing on circadian rhythms and sleep quality [36]. Yamanaka et al. compared the effects of morning and evening exercise on melatonin and core body temperature rhythms and sleep quality. They found that evening exercise (17:00-19:00) for 2 h increased nocturnal core body temperature, delayed the melatonin rhythm phase, and decreased REM sleep (min) compared to the pre-exercise baseline in healthy males [36]. In contrast, morning exercise (10:00-12:00) increased the onset and peak melatonin levels. Core body temperature and sleep quality showed no significant differences between morning and pre-morning exercises [36].
Six studies examined the effects of morning and evening exercise, with one study not comparing the effects of exercise timing, on circadian rhythms and sleep quality [32,34,35,37,39,40]. Salivary CAR and sleep quality measured using the PSQI showed no significant differences before and after an evening football match in healthy males [35]. Flausino et al., reported that 30-60 min of evening exercise did not affect sleep quality in healthy males (VO2peak = 46 ┬▒ 7) [39]. Imboden et al. reported that indoor cycling and active stretching control during the daytime for 6 weeks decreased salivary CAR and improved sleep quality measured using the PSQI compared to the pre-exercise baseline in participants with depression, although no significant changes were observed when sleep quality measured using PSG [32]. Treadmill exercise in the morning for 12 weeks improved sleep quality (increased NREM stage 3 (N3) % sleep) and reduced cortisol concentration after awakening for participants who experienced sleep disturbances [37]. Morning exercise for 60 min in normoxia and hypoxia improved total sleep time (min) and sleep efficiency (%). Additionally, only the morning hypoxia exercise group showed increased evening plasma melatonin concentrations [34]. Ten weeks of morning exercise increased morning melatonin levels and improved sleep quality in postmenopausal sedentary women with sleep disturbances [40].
Effect of exercise intensity on circadian rhythm and sleep quality
One study compared the effects of exercise intensity on circadian rhythms and sleep quality [39]. Flausino et al. assessed the effects of two exercise intensities on core body temperature and sleep quality in healthy good sleepers. The results showed that both intensity of ventilatory threshold 1 (VT1; moderate intensity) and 50% above intensity of VT1 (>50% VT1) did not negatively affect sleep quality [39]. Core body temperature after 30 min of moderate-intensity exercise and >50% moderate-intensity exercise did not change compared to the pre-exercise baseline. Core body temperature after 60 min of moderate-intensity exercise and >50% moderate-intensity exercise increased but returned to baseline levels after 120 and 30 min, respectively [39].
Eight studies investigated the effects of one exercise intensity, with one study not comparing the exercise intensities, on circadian rhythm and sleep quality [32-38,40]. Following VT1 (moderate intensity) treadmill exercise for 50 min, morning cortisol concentration decreased and sleep quality improved in participants with chronic primary insomnia [33]. Lemos et al. reported that 50% VO2max during treadmill exercise resulted in no significant differences in plasma melatonin levels compared with the no-exercise group but reduced sleep latency (min) and increased total sleep time (min) [34]. In high-intensity exercise (85% HRmax), treadmill exercise for 12 weeks improved N3 sleep (%) and reduced morning cortisol concentration after awakening in participants who experienced sleep disturbances [37]. CAR after high-intensity interval training (HIIT; four bouts of exercise for 4 min at 90-95% HRpeak with 3 min of active recovery) was higher than that after small-sided game training, which was performed at the habitual training time in non-professional male soccer players (4 bouts of exercise for 4 min at 90-95% HRpeak with 3 min of active recovery), despite being of similar intensity. Sleep quality decreased to a greater extent after HIIT than after small-sided game training [38].
Risk of bias in the studies
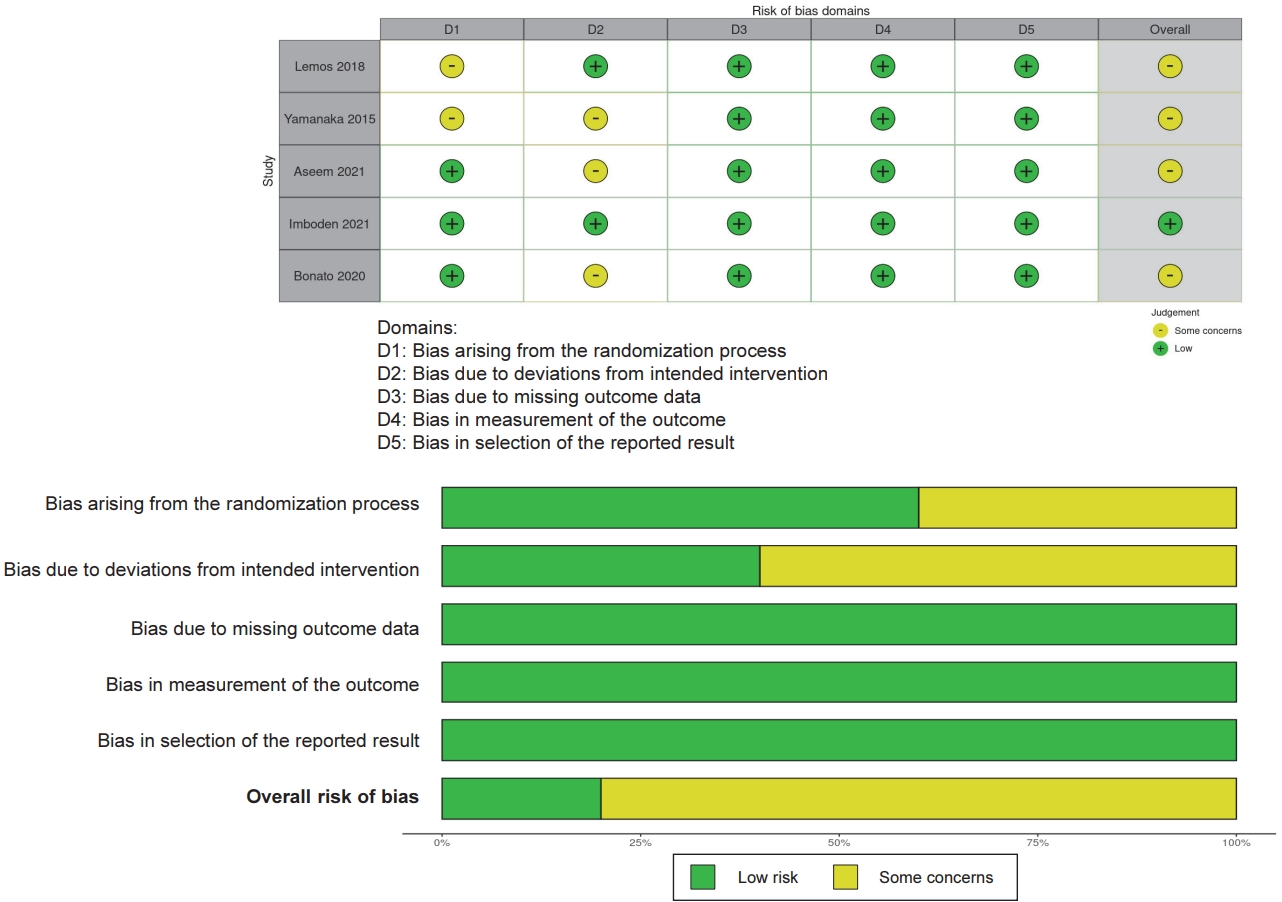
The risk of bias was evaluated separately in randomized and non-randomized controlled studies. According to the RoB2 assessment of the risk of bias in RCTs, 20% of the studies showed a low risk of bias, 80% showed some concerns about the risk of bias (moderate risk of bias). Specifically, 100% of the studies had a moderate-to-low risk of bias in the randomization process, and 40% had a low risk of bias in a deviation from the intended interventions, and 100% had a low risk of bias in the missing outcome data. In the measurement of the outcome dimension and selection outcomes, 100% had a low risk of bias. The evaluation results of each study are shown in Figure 2.
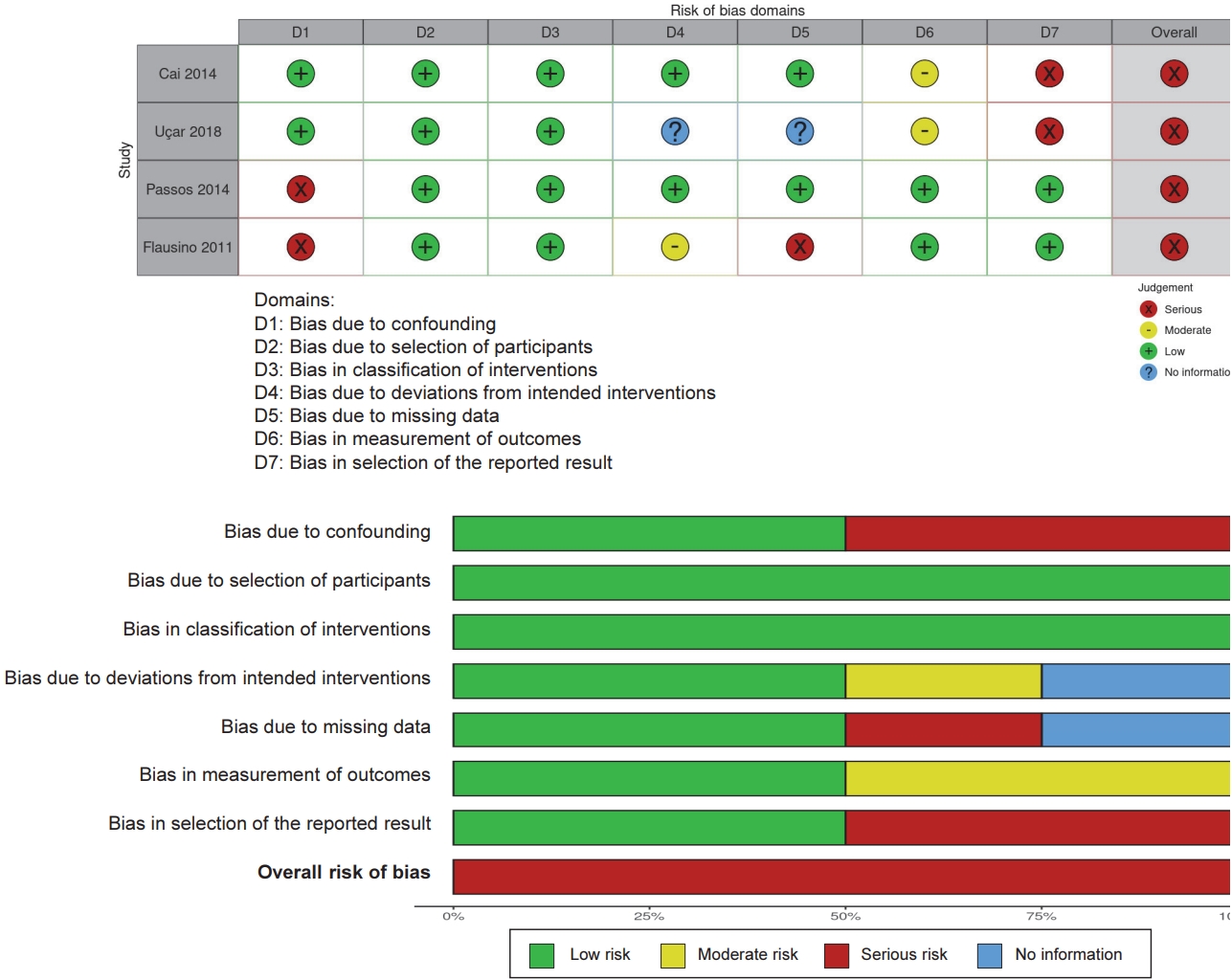
According to the ROBINS-I assessment of the risk of bias in non-RCTs, 50% of the studies had a low risk of bias in terms of confounding. Specifically, 100% had a low risk of bias in the selection of participants and classification of interventions. In a deviation from the intended interventions, 75% of the studies had a low or moderate risk of bias, and 25% of the studies had no information. Additionally, 50% had a low risk of bias, 25% had a serious risk of bias, 25% had no information regarding the missing outcome data. In the measurement of the outcome, 100% of studies had low or moderate risk of bias, 50% of the studies had low risk, and 50% had serious risk of bias in selection of the reported results. The evaluation results of each study are shown in Figure 3.
DISCUSSION
In this systematic review, we examined the effects of exercise on cortisol, melatonin, and core body temperature circadian rhythms as well as sleep quality. We found that the timing and intensity of exercise may have differing effects on physiological circadian rhythms and sleep quality.
Effect of exercise timing on circadian rhythm and sleep quality
Previous reviews and meta-analyses have indicated that morning exercise can improve sleep quality, whereas evening exercise has the opposite effect [14-16]. High-intensity, long-term exercise can prevent body temperature decrease and lead to inadequate recovery periods, thereby causing night insomnia [14]. One study examined in our review compared the effects of morning and evening exercises performed for 4 consecutive days on circadian rhythms and sleep quality. Yamanaka et al. showed that 2 h of evening exercise (17:00-19:00) for 4 consecutive days increased rectal temperature during nocturnal sleep and decreased the duration of REM sleep (min) in healthy males [36]. Melatonin offset, defined as the time when nocturnal melatonin increases and the horizontal line at 20% amplitude crosses the descending portions, was found to be delayed compared to the pre-exercise baseline in healthy males. In contrast, after morning exercise (10:00-12:00), no significant difference in sleep quality, as measured based on PSG and rectal temperature, during nocturnal sleep was observed compared to the pre-exercise baseline. The decrease in core body temperature at night is mainly attributed to an increase in heat loss from the skin of the extremities [36,41]. Yamanaka et al. reported that late-evening exercise prevented a decrease in core body temperature at night, possibly through sympathetic nerve activation, a conclusion that is supported by changes in nocturnal heart rate variability. Peripheral vasodilation, which is mediated by the autonomic nervous system, contributes to nocturnal heat loss. Evening exercise significantly increased heart rate during sleep, whereas morning exercise did not. Heart rate is stimulated by sympathetic nerve activation, and 2 h of evening exercise may continuously stimulate the sympathetic nervous system several hours after exercise. In contrast, morning exercise significantly increases very low, low, and high frequencies during sleep [36]. Although the 4-day evening exercise reduced REM sleep, no changes in NREM sleep or sleep efficiency were observed [36]. Conversely, Flausino et al. showed that 30-60 min acute evening exercise improves sleep quality [39].
Flausino et al. found an increase in core body temperature during the 60 min evening exercise [39]. However, neither exercise interfered with sleep induction. Participants in the study by Flausino et al. were good sleepers, as confirmed by clinical evaluation using the PSQI and PSG. Flausino et al. suggested that including only good sleepers in the experiment might not have any significant effect owing to little room for improvement in sleep quality, such as ceiling and floor effects [16,39]. Studies measuring the effect of evening exercise on sleep quality and circadian rhythm sleep have been either acute or short-term. Tworoger et al. reported that evening exercisers who exercised for more than 225 min for 12 months had an increased risk of reporting trouble falling asleep in postmenopausal woman [17]. In our systematic review, circadian rhythms and sleep quality according to the timing of exercise varied with exercise duration. Further research is needed to determine the effects of long-term evening exercise on circadian rhythms and sleep.
Effect of exercise intensity on circadian rhythm and sleep quality
Flausino et al. compared the effects of different exercise intensities on core body temperature and sleep quality. Both moderate exercise and >50% moderate-intensity treadmill exercise in healthy good sleepers did not negatively affect sleep quality [39]. Flausino et al. found that 60 min of VT1 (moderate intensity) and >50% VT1 intensity exercise increased core body temperature. VT1 exercise caused a mean elevation of core body temperature by 0.28┬░C that returned to baseline levels 120 min later, while >50% VT1 intensity exercise elevated core body temperature by 0.45┬░C, which returned to baseline within 30 min after exercise. Exercise did not interfere with sleep induction. Flausino et al. reported that including only good sleepers in an experiment might not result in any significant differences in sleep quality [39]. Moderate-intensity exercise for 4 months reduced salivary CAR and improved sleep quality, as measured via PSQI, in participants with depression [33]. Furthermore, acute exhaustive exercise during the daytime decreases urine cortisol after awakening, increases SWS, and decreases the 1st REM period in moderately active healthy adults (VO2max = female 39.74, male 54.9) [42]. Our review showed that acute high-intensity exercise may not significantly affect sleep quality.
However, a long-term longitudinal study reported significantly higher morning cortisol levels and reduced sleep quality after overtraining in the postseason compared to the preseason in female soccer players [43]. Continuing excessive high-intensity exercise may adversely affect sleep quality, and it is necessary to adjust the timing and intensity of exercise according to the individual. Many previous studies on the effects of exercise intensity and timing on circadian rhythms and sleep quality have involved acute exercise. Moreover, no studies have been conducted on the effects of resistance training on circadian rhythms and sleep quality. Further research is needed on the timing and intensity of long-term duration exercise and resistance training.
Effect of exercise on circadian rhythm and sleep quality in sleep disturbance
For 12 weeks, 85% HRmax treadmill exercise for 60 min in the morning improved NREM stage 3 sleep (N3 %), measured via PSG, indicating improved sleep quality, and cortisol decreased after awakening in young adults who experienced sleep disturbances (PSQI>5) [37]. Aseem et al. reported an increase in N3 sleep (%), which in turn supports the enhancement of slow waves in response to endurance exercise training [37,44]. Several studies echoed the results of our study regarding increased N3% and suggested that exercise interventions may be associated with increased deep sleep duration [45]. Furthermore, Aseem et al. reported a decrease in serum cortisol levels in the morning after aerobic exercise, which acts on the HPA-axis and downregulates cortisol levels, thereby improving sleep quality [46]. Serum melatonin levels before sleep showed no significant differences before and after exercise in young male adults who experienced sleep disturbances [37]. In participants with chronic primary insomnia, VT1 intensity treadmill exercise for 50 min decreased morning cortisol concentration and improved sleep quality [33]. Postmenopausal subjects who experienced sleep disturbances exhibited increased morning (7:30-9:00) melatonin concentration and improved sleep quality (decreased PSQI score) after 75-85% HRR group-based step aerobic exercise in the morning for 10 weeks [40]. A significant decrease in age-related melatonin levels often explains why older adults experience sleep disorders. Most studies on the association between exercise and melatonin have found that acute exercise temporarily increases melatonin levels [40,47,48]. A previous study indicated that an increase in melatonin can modulate adaptive stress responses, offering protective effects against free radical-induced damage [49]. Taken together, enhanced melatonin production in menopausal women with sleep disorders may at least partially reflect the bodyŌĆÖs adaptation to exercise-induced increases in antioxidant levels and immune system activity.
Effect of exercise on circadian rhythm and sleep quality in athletes
Compared to the general population, athletes perform more high-intensity exercise and training, in addition to several evening training sessions. In one study, non-professional athletes exhibited decreased sleep quality after high-intensity exercise and increased nocturnal or post-wakeup cortisol levels [38]. Bonato et al. reported that sleep quality after HIIT was worse than that after small-sided game training in non-professional soccer players, although the intensity of HIIT and small-sided game training are expected to be similar. Notably, increased CAR was observed only after the HIIT [38]. Bonato et al. suggested that HIIT increases cortisol release and decreases sleep quality due to psychological stress in athletes [38]. The circadian rhythm of cortisol notably increased immediately after waking, peaking within 30-45 min. This response is a neuroendocrine manifestation of the hypothalamic-pituitary-adrenal axis, which has been shown to be sensitive to psychological stressors, such as exercise. Previous observational studies have reported that netball athletes experience poor sleep quality and sleep disturbances after evening training in athletes following late night exercise [50]. This decrease in sleep quality and duration following evening exercise may be attributed to several psychophysiological factors that increase core body temperature, HR, HR variability, muscle soreness, muscle pain, and psychological stress [51].
Cortisol levels increased during the early part of the night and REM (%) decreased after moderate exercise (120-150 km, 4 h 30 min) compared with no exercise, whereas cortisol levels immediately after exercise and nocturnal time did not differ significantly between non-professional triathletes who performed low-intensity cycling (40 km, 2 h 30 min) and those who did not exercise [25]. Delayed inhibitory effects on pituitary-adrenal secretory activity were observed during sleep after a cortisol peak induced by exogenous ACTH administration [52]. Regular temporal patterns of cortisol secretion during sleep can be strongly distorted by long-duration exercise, even when the exercise was performed 4 h before sleep [25]. Kern et al. reported that peak growth hormone levels decreased during the first half of the sleep period, whereas cortisol levels were simultaneously increased. Furthermore, the reduced growth hormone to cortisol ratio during early nocturnal sleep suggests reduced anabolic function during sleep after high-intensity exercise [25].
A previous longitudinal study reported significantly higher morning cortisol levels and reduced sleep quality in athletes in the postseason, accompanied by high scores on the Soci├®t├® Franc├¦aise de Medecine du Sport Questionnaire, including severe muscle pain and tiredness, compared to the preseason. This systematic review showed that cortisol concentration and sleep quality are affected by high-intensity exercise in athletes [43]. Further studies are needed to determine the relationship between appropriate training timing and cortisol levels to improve sleep quality in athletes.
Effect of exercise on circadian rhythm depending on chronotype
Recent studies have shown that circadian rhythms respond differently to exercise depending on the individuals under study belong to the late chronotype (night owls; stay up late and feel most alert in the evening) or early chronotype (morning larks; rise early and feel their best in the morning); however, this was not considered in this systematic review owing to a lack of sleep quality data, even though these late and early chronotypes are associated with sleep quality [53,54]. Thomas et al. reported that 70% VO2peak morning exercise induces greater dim light melatonin onset phase advance shifts (0.62 ┬▒ 0.18 h) than evening exercise (-0.02 ┬▒ 0.18 h; p = 0.01), and suggested that late chronotypes may benefit from phase advancement induced by morning or evening exercise; however, evening exercise may exacerbate periodic alignment errors in early chronotypes. The study showed that morning exercise had the most potential to alleviate circadian misalignment in the late chronotype, which is often observed in young individuals [54]. The mechanism by which morning exercise results in the development of circadian rhythms remains unclear; however, it is well known that exposure to morning light can phase advance circadian rhythms [55,56]. Youngstedt et al. reported that the combination of bright light and exercise (80.8 ┬▒ 11.6 min) has a significant phase-delaying effect compared with exercise alone (47.3 ┬▒ 21.6 min), and the findings of the study suggested that late night bright light followed by early morning exercise may have a circadian phase-shifting effect [56]. Therefore, personalized exercise timing prescriptions based on chronotype can alleviate cyclical alignment errors. However, there is a dearth of research on the effects of exercise on circadian rhythm and sleep quality from the perspective of chronotypes. Therefore, it is necessary to further study the effects of exercise on sleep quality by considering individual chronotypes. With regard to melatonin, the peak stimulation levels in the body change throughout an individualŌĆÖs life [57,58]; however, a limitation of this review is that it we were unable to consider this issue owing to a lack of data. Future studies should study circadian rhythms, including those of melatonin, according to individualŌĆÖs life stage.
CONCLUSION
In this systematic review, we observed that short-term evening exercise or high-intensity exercise did not have a significant negative effect on sleep quality but physiological circadian rhythm tended to alter. Long-term morning exercise tended to decrease cortisol concentrations after awakening and improved sleep quality. Different factors, such as duration, intensity, and timing, have different effects on sleep quality. Future studies should investigate circadian hormones along with the sleep quality suitable for different individuals, as well as examine the effects of long-term exercise timing and intensity on circadian rhythms and sleep.