The COL5A1 genotype is associated with range of motion
Article information
Abstract
[Purpose]
The aim of our study was to investigate the association between COL5A1 genotype and Range of Motion as measured by the passive straight leg raise (SLR) and whole body join laxity (WBJL) in Asian population.
[Methods]
One hundred and seventy seven participants including Korean and Japanese college students (male = 109, female = 68) participated in the study. Each subject performed the passive straight leg raise and whole body join laxity test. Genotyping for the COL5A1 (rs 12722) polymorphism was performed using the TaqMan approach. The COL5A1 genotype exhibited a Hardy-Weinberg equilibrium distribution in our population.
[Results]
The physical parameters including height, weight, and BMI were higher in < 90° group than > 90° group. The SLR exhibited significant difference among the COL5A1 group. However, the WBJL did not differ significantly among the COL5A1 genotype, but significant difference was seen in CC genotype when compared to CT (2.99 ± 1.72) or TT (2.70 ± 1.52) genotype.
[Conclusion]
We concluded that COL5A1 gene polymorphism is associated with increased SLR ROM in Asian population.
INTRODUCTION
Musculoskeletal injuries can be a result of participation in sports activities or carrying out physical activities for health benefits [1]. The causes of musculoskeletal injuries result from a complex interaction of multiple risk factors and events [2]. Range of motion (ROM) has been known as one of the risk factors for increased musculoskeletal injuries [3,4]. Musculoskeletal flexibility is defined as the ability to move a joint through its complete ROM, and therefore it is important to maintain flexibility as decreased ROM is a contributing risk factor for injuries [5].
Exercises to enhance flexibility can improve overall performance of athletes by preventing injuries with subsequent increase in ROM. Moreover, many athletes and others continue with their daily physical activities to increase the rate of performance in an event and for various health benefits; at the same time they are exposed to the risk of injuries caused due to fatigue. Arnason et al. [6] established that injuries occurring during the time of training or physical activity were musculoskeletal injuries. Thus, it is important to increase flexibility or ROM for enhancement in performance and to prevent musculoskeletal injuries.
Type V collagen is a minor component of tissues containing type I collagen, such as skin, tendons, ligaments, bone, cornea, and blood vessels [7]. COL5 Va1 (COL5A1, SNP rs12722) has been located on chromosome 9 in humans [8], and SNP rs 12722 produces two alleles of the COL5A1 gene, namely, the COL5A1 rs 12722 C-and T-alleles. Recently, studies on COL5A1 have been represented 1) Ehlers-Danlos syndrome (EDS) and 2) injuries (running performance, achilles tendon injuries, and ROM). Most patients with classic EDS have disease-causing mutations within one copy of their COL5A1 genes, which results in a loss of function of the mutated gene and a 50% reduction in the production of type V collagen [9].
A common C to T single nucleotide polymorphism within the COL5A1 gene is associated with a number of sports injuries or performance-related phenotypes [10]. Posthumus et al. [11] suggested that the CC genotype of COL5A1 was under-represented in female subjects with anterior cruciate ligament ruptures. The causes of ‘‘increased risk’’ phenotype may be the result of increased musculotendinous stiffness and decreased ROM [12]. Moreover, Collins et al. [10] established that COL5A1 is independently associated with lower limb ROM in Caucasian subjects. Since the abnormal ROM has been reported to be associated with injuries, it is important to identify genetic factors for ROM.
However, association between COL5A1 genotype and ROM in Asian people is still unclear. Therefore, the aim of our study was to investigate the association between COL5A1 genotype and flexibility as measured by the passive straight leg raise (SLR) and whole body join laxity in general Asian college students.
METHODS
Participants
One hundred and seventy seven Korean and Japanese college students (male = 109, female = 68) were recruited for the present study (Table 1). The details along with the purpose and the methods of study were explained to the participants. The subjects also signed an informed consent form before participation.
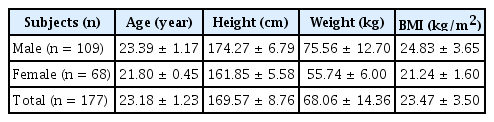
The physical characteristic of the subjects
Range of motion measurements
During muscle tightness measurement, the angle of each joint of the hamstrings and quadriceps were measured, by referring to the measurement method reported by previous study. We performed the SLR [13] test in participants, who had no preexistent or current injury in the examined leg. The SR and SLR measurement were assessed twice, and the average score was calculated.
In addition, we performed the whole body join laxity (WBJL) [14], such as wrist, knee, spine, elbow, shoulder, ankle, and hip seven positions were tested. The total of positive position was regarded as the measured value.
DNA extraction and COL5A1 genotyping
Cotton swab (Single Wrapped, COPAN, CA, USA) derived buccal cells were scraped from inner side of the cheek of participants and genomic DNA was extracted. After the cells were lysed in 400μl of DNA lysis solution and incubated at 95℃ for 3 minutes. Typically, 400μl of DNA stabilizing solution was added to the samples and stored at 4℃ until polymerase chain reaction (PCR) was carried out. Genotyping for the COL5A1 polymorphism was performed by real-time PCR using a TaqMan probe (rs12722, Pre-Designed SNP Genotyping assays). The PCR cycling reaction, using thermal cycler (7500, Applied Biosystem, CA, USA) were as follows: 95℃ for 10 min, 40 cycles at 95℃ for 15 sec and at 60℃ for 1 min.
Statistical analysis
The SPSS statistical package version 19.0 for Windows (SPSS, Inc., Chicago, IL, USA) was used to perform all statistical evaluations. Allele frequencies were determined by gene counting. X2 test was used to confirm that the observed genotype frequencies exhibited a Hardy-Weinberg equilibrium distribution. Further, we carried out an X2 test for understanding association between SLR and COL5A1 allele and Fisher’s exact test was used to evaluate association between SLR and COL5A1 genotypes. Differences in the WBJL results of ROM among the COL5A1 genotypes were tested using analysis of variance (with Tukey’s multiple comparison test). The level of significance was set at α =0.05.
RESULTS
COL5A1 polymorphism
The distribution of the COL5A1 polymorphism and allele are presented in Table 2. The distribution of COL5A1 gene in subjects was in the Hardy-Weinberg equilibrium (p = 0.159), and the results were analogous to that of the previous study in Asian population [15].
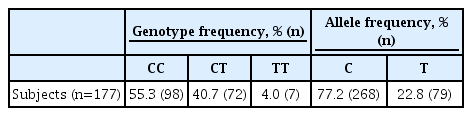
Distribution of COL5A1 genotype in all subjects
Physical characteristics of the SLR and COL5A1 gene
The characteristics of the subjects according to each genotypes and SLR are shown in Table 3. There was no significant difference among the groups with respect to genotypes (Table 3a). However, significant difference was noted between the relative SLR and characteristics of the subjects. The physical parameters including height, weight, and BMI were higher in < 90° group than > 90° group (Table 3b).

The characteristic of the subjects according to each genotype and SLR
Relationship of COL5A1 polymorphism with ROM
The SLR and WBJL results of the ROM with respect to COL5A1 genotype and the C-dominant model (CC and CT genotype) and T-dominant (TT and CT genotype) model in subjects are shown in Table 4. The relative SLR differed significantly among the COL5A1 genotype (Table 4a). However, no significant difference was seen in the WBJL among the COL5A1 genotype (Table 4b), but significant difference was seen in CC genotype when compared to CT (2.99 ± 1.72) or TT (2.70 ± 1.52) genotype.

Range of motion based on COL5A1 polymorphism
DISCUSSION
The present study is the first of its type to investigate the association between COL5A1 genotype and ROM in general Asian college students. The main finding of the study was the presence of association between SLR ROM and COL5A1. Moreover, an increasing trend in WBJL ROM was noted in subjects with COL5A1 CC genotype, which was not significant. The physical parameters including height, weight, and BMI were higher in < 90° group than > 90° group. Previously, association between COL5A1 genotypes and straight leg raise ROM in Caucasian population has been reported [16]. In addition, a positive correlation between COL5A1 genotype and ROM has been established in a group of South African participants [1]. An overexpression in CC genotype has been reported in individuals with greater ROM [17]. CC genotype collagen fiber containing large irregular and small fibrils. These mutations cause Ehlers-Danlos Syndrome (EDS), which has been demonstrated to have a detrimental effect on the habitual level of physical activity within the patients. Also, the study demonstrates presence of a mixture of large and small irregular fibrils in EDS. In addition, TT genotype collagen fibers containing smaller more densely packed fibrils have been reported. The fibrils, which are proposed to have an increased stiffness and/or creep inhibition, are associated with reduced joint ROM, increased risk for specific musculoskeletal soft tissue injuries, and faster endurance running performance. [10]. COL5A1 gene encodes ɑ1 (V) chain of type V collagen and a mutation in this gene, which causes haploinsufficiency, results in 50% reduction of type V collagen, and leads to poorly organized fibrils, decreased tensile strength, and reduced stiffness of connective [11]. It has been suggested that due to reported association with tendons, individuals with a TT genotype would have less extensible tendon structures, resulting in a lower range of motion (ROM) as compared to individuals with at least one copy of the C allele [10].
The reduction in ROM leads to concomitant reduction in physical activity [18], or an alteration in collagen integrity with increasing age [19]. Brown et al. [1] reported that SR ROM tended to increase with age in those subjects with COL5A1 CC genotype, while there was little or no correlation in the other two genotypes. Bertuzzi et al. [20] reported no significant differences between COL5A1 genotypes for ROM in physically active men. Saunders et al. [21] stated that COL5A1 genotypes might interact with age for ROM in physically active subjects. On the other hand, Goncalves-Neto et al. [22] and Satomi et al. [23] reported that damaged and pathological tendons contained relatively higher proportion of collagen type V, and these alterations were accompanied by a reduction in type I collagen. Thus, according to COL5A1 genotype might be increase rate of injuries in elderly. However, in the present study, subjects were young college students, and there were significant differences in the three COL5A1 genotypes with SLR.
The present study has some limitations. We did not consider the levels of physical activity and exercise. We assumed that there were no significant differences in physical activity levels and exercise experienced. However, physical activity and exercise levels should be considered in future studies. Another limitation is that sample size was relatively small, and further studies with larger populations are required to validate our findings. The primary aim of the study was not intended to investigate gender-specific genetic risk factors, and therefore further research is required.
In conclusion, our data indicates association between the COL5A1 genotypes and SLR in young Asian population. CC genotype of COL5A1 has been found to be associated with increased SLR ROM. Although present study shown that did not significantly in WBJL but increased tended to CC genotype. Therefore, present findings provide preliminary evidence on association of COL5A1 genotype with ROM in Asian population.
Acknowledgements
This work was supported by the National Research Foundation of Korea Grant funded by the Korean Government (NRF-2014S1A5B5A07039021).